
 Deutsch
Deutsch Nederlands
Nederlands Turkish
Turkish Russian
Russian Italiano
Italiano Français
Français Português
Português العربية
العربية
Libido and Male Health
Robert Gorter, MD, PhD, is emeritus professor of the University of California San Francisco (UCSF)
Libido and Male Health:
Dr. Robert Gorter: “Man is born as an inapt creation by Nature, being within Nature that is often aggressive towards him and yet transcending it. Man has to find and develop principles of action and decision-making which replace the principles of instincts which he shares with animals and Nature in general: a painful process from being born unfree to becoming a free individuality with all the responsibilities that come with it.”
Libido is one’s man best friend and one’s worst enemy. It is that force in us that keeps us going. One example is greed. Greed is a bottomless pit which exhausts the person in an endless effort to satisfy his needs without ever reaching satisfaction. The consequence is frustration and the basis for pathologic behavior like ruthlessness, absolute egoism and psychopathic conduct.
One can observe this everywhere around him: from destruction of the environment to killing (ISIS) systematically to warfare where a very few benefit from death and destruction of many others.
This contribution by Dr. Robert Gorter is an attempt to get closer to an understanding of what Libido is from a physiological point of view as well as from a developmental point of view.
Various Factors determining Libido:
Sigmund Freud (1856-1939) was an Austrian neurologist, psychiatrist, and a fierce criticist of society and religion. He was the founder of Psychoanalysis. Freud is considered one of the most influential thinkers of the 20th century. His theories and methods are applied till today.
Since Sigmund Freud developed his psychoanalysis towards the end of the 19th century, and defined the concept of “Libido,” much has been said and postulated about sexual function in humans and about libido
Libido is a person’s overall sexual drive or desire for sexual activity. Sex drive is determined by biological, psychological, and social factors. Biologically, levels of hormones such as testosterone affect sex drive; social factors, such as work and family, also have an impact; as do internal psychological factors, like personality and stress. Sex drive may be affected by medical conditions, medications, life style and relationship issues. A person who has extremely frequent or a suddenly increased sex drive may be experiencing hyper-sexuality, or puberty in which the body builds up chemicals and causes a higher sex drive. Asexual people may lack any sexual desires.
A person may have a desire for sex, but not have the opportunity to act on that desire, or may on personal, moral or religious reasons refrain from acting on the urge. Psychologically, a person’s urge can be repressed or sublimated. On the other hand, a person can engage in sexual activity without an actual desire for it. Multiple factors affect human sex drive, including stress, chronic fatigue, any illness, pregnancy, fashion and peer-pressure, and many others.
Sexual desires are often an important factor in the formation and maintenance of intimate relationships in both men and women, and a lack or loss of sexual desire can adversely affect relationships of all kinds. Changes in the sexual desires of either partner in a sexual relationship, if sustained and unresolved, may cause problems in the relationship. The infidelity of a partner may be an indication that a partner’s changing sexual desires can no longer be satisfied within the current relationship. Problems can arise from disparity of sexual desires between partners, or poor communication between partners of sexual needs and preferences.
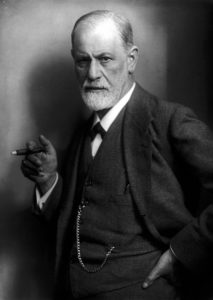
Siegmund Freud (1856-1939)
Sigmund Freud defined libido as “the energy, regarded as a quantitative magnitude … of those instincts which have to do with all that may be comprised under the word ‘love’.” And “It is the instinctive energy or force, contained in the strictly unconscious structure of the psyche.”
Freud developed the idea of a series of developmental phases in which the libido fixates on different erogenous zones—first in the oral stage (exemplified by an infant’s pleasure in nursing), then in the anal stage (exemplified by a toddler’s pleasure in controlling his or her bowels), then in the phallic stage, through a latency stage in which the libido is dormant, to its reemergence at puberty in the genital stage. (Karl Abraham would later add subdivisions in both oral and anal stages). Freud pointed out that these libidinal drives can conflict with the conventions of civilized behavior, represented in the psyche by the superego. It is this need to conform to society and control the libido that leads to tension and disturbance in the individual, prompting the use of ego defenses to dissipate the psychic energy of these unmet and mostly unconscious needs into other forms. Excessive use of ego defenses results in neurosis. A primary goal of psychoanalysis is to bring the drives of the id into consciousness, allowing them to be met directly and thus reducing the patient’s reliance on ego defenses.
Freud viewed libido as passing through a series of developmental stages within the individual. Failure to adequately adapt to the demands of these different stages could result in libidinal energy becoming ‘dammed up’ or fixated in these stages, producing certain pathological character traits in adulthood. Thus, the psychopathologized individual for Freud was an immature individual, and the goal of psychoanalysis was to bring these fixations to conscious awareness so that the libido energy would be freed up and available for conscious use in some sort of constructive sublimation.
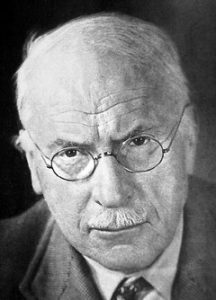
Carl Jung (1875-1961)
According to Swiss psychiatrist Carl Gustav Jung, the libido is identified as psychic energy. Duality (opposition, polarity) that creates the energy (or libido) of the psyche, which Jung asserts expresses itself only through symbols: “It is the energy that manifests itself in the life process and is perceived subjectively as striving and desire.”
Defined more narrowly, libido also refers to an individual’s urge to engage in sexual activity, and its antonym is the force of destruction termed mortido or destrudo.
Psychological factors:
Psychological factors can increase or reduce the desire for sex. Usually, factors that reduce the desire for sex can include lack of privacy or intimacy, stress or fatigue, distraction or depression.
Environmental stress, such as prolonged exposure to elevated sound levels or bright light, can also affect libido. Other causes include experience of sexual abuse, assault, trauma, or neglect, body image issues and anxiety about engaging in sexual activity.
Psychological factors that can increase the desire (drive) for sex are through increased feeling of well-being and success, feeling to be liked (adored, narcissism), wanting to be dominating, etc. (“who penetrates is in control”).
Physical factors:
Physical factors that can affect libido include: endocrine issues such as hypothyroidism, levels of available testosterone in the bloodstream of both women and men, the effect of certain prescription medications (for example flutamide or beta-blockers), various lifestyle factors and the attractiveness and biological fitness of one’s partner. Inborn lack of sexual desire, often observed in asexual people, can also be considered a physical factor. In males, the frequency of ejaculations affects the libido. If the gap between ejaculations is long, there will be a stronger desire for sexual activity. Long-time abstinence can also decrease the sexual drive.
Being very underweight or malnourished can cause a low libido due to disruptions from normal hormonal levels.
Anemia is particularly a cause of lack of libido in women due to the loss of iron during strong menstruation (hypermennhorrea).
Smoking, alcohol- and drug abuse may also cause disruptions in the hormonal balances and therefore, lead to a decreased libido. Moreover, specialists suggest that several lifestyle changes such as exercising, quitting smoking, lower or stop consumption of alcohol or using prescription drugs may help increase one’s sexual desire. Learning stress management techniques can be helpful for individuals who experience libido impairment due to a stressful life.
Aphrodisiacs are known to increase individuals’ libido due to either their chemical composition or their pharmacologic effects (Viagra, oxytocin).
Males reach the peak of their sex drive in their late teens, while females reach it in their thirties. The surge in testosterone hits the male at puberty resulting in a sudden and extreme sex drive which reaches its peak in early adolescence, and then drops slowly over his lifetime. In contrast, a female’s libido increases slowly during adolescence and peaks in her mid-thirties. Actual testosterone and estrogen level, which affect a person’s sex drive, can vary considerably.
Sexual desire disorders:
There is no widely accepted measure of what is a healthy level for sex desire. Some people want to have sex every day, or more than once a day; others once a year or not at all. However, a person who lacks a desire for sexual activity for some period of time may be experiencing a hypoactive sexual desire disorder or may be asexual. A sexual desire disorder is more common in women than in men. Erectile dysfunction can only occur in men and may be a cause for the lack of sexual desire; however, these two should not be confused. Moreover, specialists have brought to attention that libido impairment may not even occur in cases of men with erectile dysfunction. However, men can also experience a decrease in their libido as they age.
The American Medical Association (AMA) has estimated that several million US women suffer from a female sexual arousal disorder, though arousal is not at all synonymous with desire, so this finding is of limited relevance to the discussion of libido. Some specialists claim that women may experience low libido due to some hormonal abnormalities such as lack of luteinizing hormone or androgenic hormones, although these theories are still controversial. Also, women commonly lack sexual desire in the period immediately after giving birth. Moreover, any condition affecting the genital area can make women reject the idea of having intercourse. It has been estimated that half of women experience different health problems in the area of the vagina and vulva, such as thinning, tightening, dryness or atrophy. Frustration may appear as a result of these issues and because many of them lead to painful sexual intercourse, many women prefer not having sex at all. Surgery or major health conditions such as arthritis, cancer, diabetes, high blood pressure, coronary artery disease or infertility may have the same effect in women. Surgery that affects the hormonal levels in women include oophorectomies (removal of the ovaries).
Hypersexuality:
While some people mistakenly think that hypersexual disorders and sex addiction merely refers to an unusually high sex drive, it is much more complex than that. It is very similar to other addictions, which is evident upon closer examination of the various sex addiction signs.
Just as an alcoholic craves his next drink, thinks he can stop on his own but fails over and over, uses alcohol to ease emotional pain, stress, loneliness, and anxiety, and continues to drink despite the negative consequences, so it is with a sex addict. Like other addictions, sex addiction is also progressive. It often starts with a relatively harmless behavior such as excessive masturbation while watching porn. Over time, however, it typically leads to other types of sexual activity that may be very risky or blatantly dangerous.
For the sex addict, sexual activity provides an intense, intoxicating euphoria or “high” while lacking any genuine emotional connection, intimacy, or love. It’s a temporary escape. Once the high wears off, the vicious cycle starts all over again. For the addict, the activity is not fulfilling. It has a significant negative impact on his life and often causes a lot of shame and self-loathing.
The indicators of hypersexual disorders will vary to some degree depending on the individual. For example, some sex addicts have multiple extramarital affairs, while others frequently hire prostitutes or use phone- of cyber-sex services excessively. Following are some of the most common sex addiction signs:
- Excessive masturbation – This is one of the most common early sex addiction signs. Often the sex addict masturbates while engaging in other sexual activity (e.g. while viewing pornography or talking to a phone sex operator).
- Obsessing about sex to the point that it interferes with their life
- Spending a significant amount of time planning their sexual activity – Sex addicts, just like drug addicts and other types of addicts, will devote a large amount of time determining where and how they will get their next “fix”.
- Frequent viewing of pornography or use of sexually explicit websites or other online services – This may include videos, adult magazines, pornographic websites, “adult” chat rooms, paying to watch sexual activity via webcams, or using dating websites that connect people interested in sexual relationships and / or one night stands.
- Having multiple extramarital affairs or frequently having sex with multiple partners
- Frequent one-night stands with total strangers or prostitutes
- Staying emotionally detached from sexual partners – Many sex addicts are unable to establish a normal, healthy connection with a sexual partner. This is often due to deep-seated feelings of self-hate and shame. It’s not uncommon for a sex addict to want nothing more to do with a sexual partner once the activity is over.
- Frequent sex without using protection – Many sex addicts engage in high risk behavior such as unprotected sex. This is often because they are so driven to satisfy their craving that they don’t consider or care about the potential consequences. Or, they like the excitement and adrenaline rush of the “Russian Roulette” feeling
- Engaging in sexual behavior that directly conflicts with their personal values or religious beliefs – For example, sex addiction signs for someone who is a devout Christian or Catholic may include having multiple partners or extramarital affairs, frequent one night stands, sex with children, or sex with prostitutes. They believe their behavior is morally wrong yet they’re unable to stop (neurosis).
- Obsessing about a sexual partner who is unattainable – This type of fixation may lead to stalking or sexually harassing the individual, spying on them bathing or engaging in sexual activity (voyeurism), and, in some instances, stalking and violence.
- Frequently engaging in paraphilias (sexual behaviors that are considered unusual, distasteful, or unacceptable) – Paraphilias include things like exhibitionism, voyeurism, sadism, masochism, and pedophilia. Although they may indicate a possible addiction, not everyone who engages in paraphilias is a sex addict.
- The inability to stop despite the consequences – As with all addictions, this is one of the primary sex addiction signs. The vast majority of sex addicts are unable to stop without treatment for their addiction.

Exaltation
Orgasm (from Greek ὀργασμός orgasmos “excitement, swelling”; also sexual climax) is the sudden discharge of accumulated sexual tension during the sexual response cycle, resulting in rhythmic muscular contractions in the pelvic region characterized by sexual pleasure. Experienced by males and females, orgasms are controlled by the involuntary or autonomic nervous system. They are often associated with other involuntary actions, including muscular spasms in multiple areas of the body, a general euphoric sensation and, frequently, body movements and vocalizations are expressed. The period after orgasm (known as a refractory period) is often a relaxing experience, attributed to the release of the neuro-hormones like oxytocin and prolactin, as well as endorphins (or “endogenous morphine”).
Human orgasms usually result from physical sexual stimulation of the penis in males (typically accompanying ejaculation), and the clitoris and “G” spot in females. Sexual stimulation can be by self-practice (masturbation) or with a sex partner (penetrative sex, non-penetrative sex, or other sexual activity).
The health effects surrounding the human orgasm are diverse. There are many physiological responses during sexual activity, including a relaxed state created by prolactin, as well as changes in the central nervous system such as a temporary decrease in the metabolic activity of large parts of the cerebral cortex while there is no change or increased metabolic activity in the limbic (“bordering”) areas of the brain. There is also a wide range of sexual dysfunctions, such as anorgasmia. These effects impact cultural views of orgasm, such as the beliefs that orgasm and the frequency/consistency of it are important or irrelevant for satisfaction in a sexual relationship, and theories about the biological and evolutionary functions of orgasm.
Orgasm in non-human animals has been studied significantly less than orgasm in humans, but research on the subject is ongoing.
In males, orgasms can be achieved by a variety of activities: sufficient sexual stimulation of the penis can be achieved during vaginal or anal intercourse, oral sex (fellatio), non-penetrative sex or masturbation. In women, sufficient sexual stimulation can be achieved during vaginal intercourse, oral sex (cunnilingus), non-penetrative sex or masturbation. Orgasm may also be achieved by the use of a sex toy, such as a sensual vibrator or an erotic electrostimulation. It can additionally be achieved by stimulation of the nipples, uterus, or other erogenous zones, though this is rarer.
Oxytocin is a mammalian neuro-hypophysial hormone. Produced by the hypothalamus and stored and secreted by the posterior pituitary gland, oxytocin acts primarily as a neuromodulator in the brain.
Oxytocin plays an important role in the neuroanatomy of intimacy, specifically in sexual reproduction of both sexes, in particular during and after childbirth; its name comes from Greek ὀξύς, oksys “swift” and τόκος, tokos “birth.” It is released in large amounts after distension of the cervix and uterus during labor, facilitating birth, maternal bonding, and, after stimulation of the nipples, lactation. Both childbirth and milk ejection result from positive feedback mechanisms.
Recent studies have begun to investigate oxytocin’s role in various behaviors, including libido and orgasm, social recognition, pair bonding, anxiety, and maternal behaviors. For this reason, it is sometimes referred to as the “bonding hormone”. There is some evidence that oxytocin promotes ethnocentric behavior, incorporating the trust and empathy of in-groups with their suspicion and rejection of outsiders. Furthermore, genetic differences in the oxytocin receptor gene (OXTR) have been associated with maladaptive social traits such as aggressive behavior.
It is on the World Health Organization’s List of Essential Medicines, a list of the most important medications needed in a basic health system.
Testosterone is for men, and estrogen is for women: for the most part this is correct but there is estrogen found in all men, and women do need small amounts of testosterone. There is, however, a growing need to understand the effects of estrogen in men. Like all hormones, estrogen needs to be kept in balance in both men and women. Chronic health conditions are more likely to occur in men as a result of estrogen levels becoming too high.
Testosterone and estrogen are actually very closely related in the body. A look at their chemical structure reveals only subtle differences. Yet, the differences of the effects of these two hormones on the body are substantial. Testosterone affects nearly every cell in the male body. It improves muscle mass and bone density and will also have a positive effect on the heart, brain and blood vessels. Estrogen is actually made from the circulating testosterone in the body by an enzyme called aromatase. As men age, they tend to make increasing levels of estrogen with decreased production of testosterone. Estrogen can be made in the liver, muscle and brain, as well as the fat cells. This is actually where much of the concern lies. As obesity rates go up in this country and around the world, the production of estrogen will also increase from the fat cells. This is a bad combination of decreasing testosterone and increasing estrogen.
Males with sex chromosome genetic conditions, such as Klinefelter’s syndrome, will have a higher level of estradiol. Estradiol at higher serum levels suppress male sexual function with loss of libido, erectile function and decreased spermatogenesis.
The “normal” range of testosterone levels is quite broad, which is one of the reasons why an excess or deficiency is difficult to detect. The average adult male has somewhere between 260 and 1,000 nanograms (ng) of testosterone per deciliter (dl) of blood plasma. For comparison, the range for women is approximately 50 to 70 ng/dl.
While some reference ranges consider male testosterone levels as low as 193 ng/dL to be considered adequate, Life Extension recommends a “moderately youthful” range of between 700 and 900 ng/dL.
Each person’s body chemistry is different, such that a person whose testosterone level is at the low end of the range may still have what is needed for development. On the other hand, someone whose testosterone level is at the high end of the range may still have a slight deficiency with respect to his (or her) “normal” level. In addition, for most men, testosterone secretion surges about eight times per day, with the highest peak around 8 am and the lowest level around 10 pm. Men’s testosterone levels do not seem to have a lunar or monthly cycle.
Determining what is “normal” is a critical aspect of hormone therapy so that a deficiency or excess can be treated appropriately. Unfortunately, a baseline representing the normal healthy state is rarely available, and the average age-related decline in male testosterone is so slow that it can be difficult to recognize an imbalance. The manifestations of such an imbalance typically depend on the person’s age, as well as the severity and duration of the imbalance.
The reality of a male menopause or “andropause” is gradually gaining recognition. Men do experience hormonal changes as they age, and they usually begin to notice these changes around age 40. However, just as women can begin menopause at an earlier age, men can begin to experience changes sooner than that as well.
Between the ages of 25 and 50, a man’s testosterone level decreases by approximately 50%, while his estrogen levels, specifically estradiol, increase by 50%. The yin-yang balance still exists, but its shift results in a variety of symptoms
There is no doubt that testosterone is the key to male sexuality. However, sexuality is far more complex than that; it is complicated by several interrelated factors; including the fact that testosterone also affects the brain, influencing sexual interest, attraction, and arousal.
Sex hormones can have on the following eight separate aspects of human sexuality:
- Sexual interest or libido is related to spikes in testosterone levels reaching brain receptors.
- Attraction and arousal can be linked with male and female body odors or pheromones. A male who is low in testosterone will no longer be as pungent after a workout.
- Sexual receptivity is at its height for women when estrogen levels peak during the menstrual cycle. Men’s receptivity is not cyclical, but is more closely related to sexual function.
- Sexual function for men is not as dependent upon testosterone as it is on nitric oxide, which is what keeps the blood vessels in the penis open. However, estrogen and testosterone both play a role in women, which is to maintain the lubrication, sensitivity, and integrity of the vagina, labia, and clitoris.
- Sexual pleasure and sensitivity are heightened for both sexes when testosterone levels peak.
- The experience of sexual orgasm is enhanced for both men and women by testosterone. The pituitary hormone oxytocin rises dramatically as well, enhancing skin and sexual organ sensitivity.
- Sexual fulfillment is accomplished by the rise in oxytocin (sometimes called the “touchy, feely” hormone). Oxytocin is enhanced by estrogen and antagonized by a high testosterone level.
- Finally, sexual bonding, or love and marriage, is mediated in women by the estrogen-induced enhancement of oxytocin. For men, testosterone activates the pituitary hormone vasopressin, which causes them to pursue females and become territorial.
Thus, sex hormone imbalances can affect multiple aspects of sexuality, with a domino-like effect. In men, one of the first signs of a testosterone deficiency is a diminished libido, which can lead to problems with sexual function and fulfillment, which then further compounds the problem because these are often tied to a man’s sense of overall well-being and self-worth.
Estrogen is considered a female hormone that belongs to a set of molecules known as steroid hormones. It is produced in the ovaries of women and little amounts are made in the testes, adrenal and pituitary glands of males. Men usually have low levels of estrogen and a number of undesirable symptoms can result when levels of estrogen are too high. Measures should be taken to lower estrogen this’s too high.
Symptoms of High Estrogen (Estradiol) in Men:
- Gynecomastia/Male breast growth
The growth of male breasts is called gynecomastia. When estrogen is present in high levels in men, the cells in breasts change their behavior. They begin to grow and this leads to the breasts becoming larger and more firm instead of the distinct pectoral fat deposits most men have. This condition can occur in around half of boys in puberty, but if it continues into adulthood, there may be an underlying reason.
- Lower sex drive
Men who have high levels of estrogen may have a problem known as erectile dysfunction. This means he is unable to maintain an erection. Any man who is experiencing sexual problems should talk to his doctor about a possible hormone imbalance.
- Infertility
A man’s fertility is determined by the number of sperm he has, the movement of the sperm and whether they can survive long enough to reach and fertilize an egg. Men who are exposed to high levels of estrogen have a higher rate of infertility than men who are not. This is because estrogen lowers the sperm’s mobility.
- Stroke risk
Because excess estrogen may cause blood clots, if a man has too much estrogen in his system, he may be at a higher risk of having a stroke.
- Heart attack
The bodies of older men produce less testosterone. This causes a hormonal imbalance with estrogen becoming more dominant. An imbalance like this is often overlooked as a possible cause of cardio disease.
- Prostate problems
High levels of estrogen in men can cause differing results. Some studies show that excess estrogen may cause prostate cancer, but once the cancer occurs, the estrogen may have some anticancer activities.
- Weight gain
High estrogen levels in men can cause weight gain and that weight gain may cause higher levels of estrogen. It is a cycle that is not easily broken.
How to Lower Estrogen in Men:
- Alcohol Consumption
Alcohol causes the body to make more estrogen. The kidneys remove excessive estrogen from the body and alcohol also interferes with that process. So abstinence of alcohol will lower the estrogen (estradiol) levels in men.
- Xenoestrogens
Xenoestrogens are man-made endocrine disruptors that copy the actions of estrogen in a body. Often found in household items, they could be the cause for the growing problem of excess estrogen in men. Meat and dairy products that are raised using growth hormones, pesticides or herbicide that are eaten on food, some types of plastic products and some health and beauty products are common sources.
- Avoid soya products
Soy contains isoflavones and these raise estrogen levels in the body while lowering testosterone. Foods like soy milk, tofu and any product with soy should be avoided to help lower the levels of estrogen in men.
- Maintain a healthy weight
Estrogen is stored in fat cells and this form a reservoir of estradiol, so one of the most common causes of estrogen dominance in men is obesity, which makes maintaining a healthy weight essential.
- Exercise
Exercise lowers the amount of fatty tissue in the body and this slows the metabolism of testosterone into estrogen. Men who have high estrogen levels can benefit from regular exercise to lower these levels.
- Zinc supplementation
Zinc can slow the change of testosterone into estrogen so taking a zinc supplement can help lower the level of estrogen in a man’s body. Other antioxidants will also help slow the conversion of testosterone.
- Nuts
Another way to lower estrogen levels is to consume nuts. The fat in nuts, such as brazil nuts, almonds, cashews, walnuts, and sunflower seeds, help raise the level of testosterone in the body.
- Broccoli
Broccoli contains one of the strongest anti-estrogen supplements, DIM, so eating broccoli more often will help to lower the level of estrogen in the body. It helps the body process estrogen so the kidneys do not have to do all the work.
- Hormone replacement therapy
Hormone replacement therapy is also an option. This can come in a variety of medications like gelatin capsule pills, topical creams and gels, pellets and skin patches. The pellet type is inserted under the skin by a doctor. Best form is though is the biweekly intramuscular injection of a testosterone depot.
Circadian Rhythm of Serum Testosterone and Its Relation to Sleep: Comparison with the Variation in Serum Luteinizing Hormone, Prolactin, and Cortisol in Normal Men.
AKIHIKO MIYATAKE, YASUHIKO MORIMOTO, TATSUO OISHI, NOBUO HANASAKI, YOSHIRO SUGITA, SUSAMI IIJIMA, YOSHIO TESHIMA, YASUO HISHIKAWA, and YUICHI YAMAMURA
*Presented in part at the 14th International Conference for Chronobiology, Hannover, Germany, and the Sixth International Congress of Endocrinology, Melbourne, Australia*.
*Osaka University School of Medicine, Fukushima 1-1-50 Fukushima-ku, Osaka 553, Japan.
First Published Online: July 01, 2013
Abstract:
Frequent samples of blood were obtained for serum testosterone, LH, PRL, cortisol, and GH determinations in healthy men while awake and during nocturnal and daytime sleep. The results were correlated with polygraphic monitoring of the electroencephalogram, electro-oculogram, and electromyogram. The mean serum levels of testosterone and PRL during non-rapid eye movement (NREM) sleep and rapid eye movement (REM) sleep differed significantly from those during the waking period. However, the mean levels of these hormones during REM sleep were not statistically different from those during NREM sleep. Through all states of waking and sleep, the mean level of LH remained unchanged.
When the periods of nocturnal sleep were divided into four 3-hour periods, namely 20.00–23.00 hour (A), 23.00–02.00 hour (B), 02.00–05.00 hour (C), and 05.00–08.00 hour (D), testosterone was significantly increased during period D (P < 0.05). LH levels were similar in all four periods. The PRL level was significantly elevated during periods C (P < 0.01) and D (P < 0.01). When the nocturnal waking state was also divided into the same four time periods, testosterone was significantly elevated in period D (P < 0.05). In contrast, neither an increase in PRL nor any change in LH was seen during the nocturnal waking state. A marked elevation of cortisol was seen in period D (P < 0.01) both during the nocturnal sleeping and the nocturnal waking states.
During acute sleep-wake cycle reversal performed in two subjects, PRL was elevated during sleep in the daytime, but testosterone was not significantly altered. The GH level in these two subjects increased during the deep NREM stages during both nocturnal and daytime sleep.
The present findings suggest that the rise in the serum level of testosterone during the early morning is not directly related to sleep or to any of the sleep stages or to the changes of LH or PRL, but may be derived from an endogenous circadian rhythm similar to that of cortisol. In other words: surge of testosterone early morning causing early morning erections and incarnate again into the physical body and wake up.
This suggests strongly that testosterone initiates the re-incarnating process from around 03.00 hour on till awakening around 07.00 hour.
Note that the clock times are relative to one’s lifestyle and environment, most importantly when one is asleep, works and sees daylight. Think of the clock times as averages for a regular individual in the US and the EU who works from 09.00 to 17.00 and is asleep from 23.00 hour to 07.00 hour.
The testosterone to cortisol ratio or the T/C ratio is commonly used as a marker of tissue anabolism and tissue repair, and a can be a measure of overtraining (cortisol = “stress hormone”) goes up. As you can extrapolate from the above graphs, the T/C ratio is highest in the afternoon and evening. During this period, exercise causes the smallest increase in cortisol and the largest increase in testosterone. Cortisol elevation also recovers fastest at that time. It is very plausible that the hormonal milieu in the late afternoon is optimal for maximum muscle anabolism. However, the research is still contentious about how transient fluctuations in hormone concentrations relate to muscle growth.
Regardless of whether it is hormone-related or not, muscle hypertrophy signaling is much higher late in the afternoon and early evening than in the morning according to gene expression and cellular activation research.
A health young man and male body builder should have multiple early-morning erections as a sign of a surge of his own (endogenous) testosterone production as a way to incarnate into the physical body and wake up again.
Circadian Core Body Temperature
Much less contentious are the effects of your core body temperature. Core body temperature is the temperature at which our inner organs operate. Enzymatic reactions and one’s immune system are extremely sensitive to minor variations in the core body temperature (usually measured rectally). For the biological systems involved in high intensity physical exercise, the optimal temperature is relatively high. Core body temperature is low at night, rises quickly upon awakening and reaches a maximum in the early evening (see graph below).
The optimal body temperature for strength training normally occurs in the late afternoon to early evening 15.30 till 20.30. During this time window of four hours, one has an optimal nerve conduction velocity, joint mobility, glucose metabolism and muscular blood flow. This improves tissue stress distribution, so that your muscles can be maximally and equally activated and your connective tissue (tendons) remains healthy.
Cancer patients always have a significantly lower core body temperature and practically no circadian rhythm.
It is no surprise then that most sports records are broken in the early evening. More importantly, a multitude of randomized, controlled, trials support exercising in the late afternoon to early evening. At this time, flexibility, power and muscular strength reach their daily peak. Endurance capacity seems to have a less pronounced circadian rhythm.
Over a period of 14 months, sexual activity, both sexual intercourse and masturbation, was recorded every day, in five males (26–32 years), synchronized with lights-on at 0700 ± 1 hour and lights-off at 23.00 ± 1.5 hour to control and synchronize the melatonin production. Circadian rhythms of plasma testosterone (among other hormonal variables) were documented every month during the same time span (sampling at 4-hour intervals, for 28 hour, on test days). The circadian rhythms for sexual activity and early morning erections were computed on a monthly basis, during the year, show two prominent peaks located in the late evening and early morning (and a minor peak in the early afternoon). There was a clear autumnal peak in plasma testosterone 24-hour mean level which explains the stark increased need for sexual activity (especially for more frequent masturbation).

Derek Poundstone Record
So: what is the best time to work out?
1) Based on the circadian rhythm of your hormones, gene expression and your core body temperature, the best time to schedule your extreme training sessions is between 15:30 and 20:30. If your sessions last longer than an hour, train a bit earlier. This advice is based on the assumption that you generally sleep when it’s dark and are awake when it’s light outside (to have a well-established melatonin production).
2) Multiple early morning erections are a sign of a strong endogenous testosterone production, and a well-established circadian rhythm (which is a sign of good health and a strong condition).